Educational content. This article does not replace consultation with a doctor or pelvic physiotherapist. For persistent symptoms or pre-existing conditions, seek professional guidance before starting any exercise routine.
The pelvic floor is probably the most important muscle group you have never trained. Invisible, silent and often ignored, it is directly responsible for functions that define a man's quality of life: erection, ejaculation, urinary continence and postural stability.
Understanding the anatomy of these muscles is the first step toward understanding why strengthening them can transform your sexual health, and why Ritmo was built specifically to train this region.
What the male pelvic floor is, the direct answer
The muscular base of the pelvis
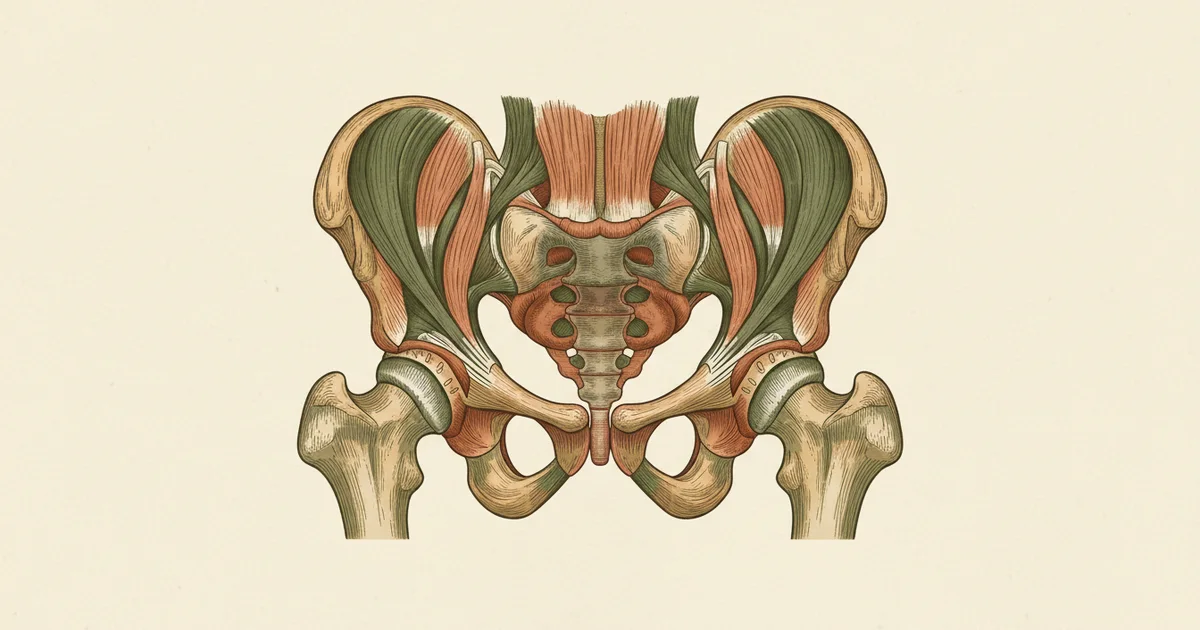
The male pelvic floor is the group of muscles that stretches from the pubic bone to the coccyx, forming the base of the pelvis. It includes the levator ani (pubococcygeus, puborectalis, iliococcygeus), the bulbocavernosus and the ischiocavernosus. These muscles directly control erectile rigidity, the ejaculatory reflex and urinary continence. When they weaken, sexual and urinary function is compromised.
Anatomy: which muscles form the pelvic floor
The male pelvic floor is a structure shaped like a muscular net that stretches from the pubic bone (at the front) to the coccyx (at the back), forming the base of the pelvis. It is made up of three layers with distinct functions:
Deep layer: Levator ani
The levator ani is the main muscle of the pelvic floor, divided into three portions:
- Pubococcygeus (PC): runs from the pubic bone to the coccyx. It is the muscle you contract when you interrupt your urine stream. It controls urinary flow and takes part in the ejaculatory reflex.
- Puborectalis: wraps around the rectum like a sling. It maintains fecal continence and contributes to the stability of the floor.
- Iliococcygeus: the most lateral and thin portion. It gives structural support to the pelvic floor as a whole.
Superficial layer: the erection muscles
- Bulbocavernosus (bulbospongiosus): wraps around the base of the penis and the urethral bulb. When it contracts, it compresses the drainage veins of the penis, preventing blood from escaping during an erection. It is also responsible for the rhythmic contractions of ejaculation.
- Ischiocavernosus: inserts into the root of the corpora cavernosa. Its contraction increases intracavernous pressure, contributing directly to erectile rigidity, especially in the full erection phase.
A direct role in erectile rigidity
Electromyography (EMG) research confirmed that the ischiocavernosus and bulbocavernosus muscles activate automatically during an erection, and that men with erectile dysfunction show significantly lower activation of these muscles.
Lavoisier P, Courtois F, Barres D, Blanchard M. Correlation between intracavernous pressure and contraction of the ischiocavernosus muscle in human penile erection. Journal of Urology. 1986; 136(4):936-939.
External urethral sphincter
It voluntarily controls the opening of the urethra. It is essential for urinary continence, especially after prostate surgery, when the internal sphincter may be compromised.
What these muscles control in practice
- Erection: the bulbocavernosus and ischiocavernosus muscles keep blood inside the corpora cavernosa. Without them, an erection may exist but lack enough firmness. See erectile dysfunction: exercises backed by science.
- Ejaculation: the ejaculatory reflex depends on rhythmic contractions of the bulbocavernosus. The ability to voluntarily control this muscle is directly linked to ejaculatory control. Learn more in premature ejaculation: causes and natural treatment.
- Urinary continence: the pubococcygeus and the external urethral sphincter work together to keep the urethra closed.
- Core stability: the pelvic floor works in synergy with the diaphragm, the transverse abdominis and the multifidus to stabilize the lumbar spine.
What causes the weakening
Unlike the biceps or the abs, the pelvic floor is rarely trained consciously. Over time, several factors contribute to its weakening:
Aging
From age 40 on, there is a progressive decline in skeletal muscle mass (sarcopenia), which also affects the pelvic floor. Studies estimate a loss of 1 to 2% of pelvic muscle strength per year after age 50.
Sedentary lifestyle and prolonged posture
Sitting for long periods compresses the pelvic floor and reduces its circulation. The muscles fall into functional disuse: they are not demanded, they do not adapt, and they gradually atrophy. A problem especially common in those who work seated all day.
Obesity
Excess weight increases chronic intra-abdominal pressure on the pelvic floor. Studies link a high BMI to a greater prevalence of incontinence and erectile dysfunction in men.
Prostate surgery
Radical prostatectomy is the most direct cause of damage to the male pelvic floor, as it can affect the nerves and muscles that control continence and erection.
Recovery after prostatectomy
Men who started pelvic floor exercises right after radical prostatectomy recovered urinary continence significantly faster than the control group, with clear differences appearing as early as 1 month after surgery.
Geraerts I, Van Poppel H, Devoogdt N, Joniau S, et al. Influence of preoperative and postoperative pelvic floor muscle training compared with postoperative PFMT on urinary incontinence after radical prostatectomy. European Urology. 2013; 64(5):766-772.
Signs that your pelvic floor needs attention
- Urine dribbling after urinating (post-void).
- Erections less firm than usual.
- Difficulty controlling ejaculation.
- A sensation of "heaviness" or pressure in the pelvic region.
- Urinary urgency: a sudden, intense need to urinate.
- Pain or discomfort in the perineum (between the scrotum and the anus).
If you relate to any of these signs, pelvic floor training is the most accessible and proven starting point. To learn the technique, see male Kegel exercises: the complete guide.
Why strengthening makes a difference, and how Ritmo helps
The good news: just like any muscle, the pelvic floor responds to training. Multiple clinical trials have demonstrated:
- Improvement of up to 75% in erectile rigidity within 3 months.
- Increase of more than 4x in ejaculatory control time.
- Faster recovery of continence after prostatectomy.
The challenge is that these muscles are internal, you do not see them in the mirror. Unlike a squat or a push-up, it is hard to tell whether you are contracting correctly, whether you are progressing, or whether you are overtraining.
That is exactly why Ritmo exists: guided 5 to 10 minute workouts that isolate each pelvic floor muscle, with automatic progression and clear instructions to make sure you are on the right track. The same protocols validated in clinical studies at European universities, adapted to fit into your daily routine.
Frequently asked questions
What is the male pelvic floor?
The male pelvic floor is the group of muscles that stretches from the pubic bone to the coccyx, forming the base of the pelvis. It includes the levator ani (pubococcygeus, puborectalis, iliococcygeus), the bulbocavernosus and the ischiocavernosus. These muscles directly control erectile rigidity, the ejaculatory reflex and urinary continence.
How do I know if my pelvic floor is weak?
The most common signs are post-void urinary dribbling, less firm erections, difficulty controlling ejaculation, a sensation of pelvic heaviness and urinary urgency. If you relate to two or more signs, pelvic training is the recommended starting point.
Which pelvic floor muscles control the erection?
The ischiocavernosus and the bulbocavernosus. They contract around the base of the penis during an erection, compressing the drainage veins and keeping intracavernous pressure high. EMG research (Lavoisier 1986) confirmed that men with erectile dysfunction show significantly lower activation of these muscles.
What causes pelvic floor weakening in men?
Aging (sarcopenia after age 40, with a 1 to 2% loss of pelvic strength per year after age 50), a sedentary lifestyle, prolonged sitting posture, obesity (chronic intra-abdominal pressure), prostate surgery and chronic stress (hypertonicity).
Is it worth strengthening the pelvic floor?
Yes. Studies show an improvement of up to 75% in erectile rigidity within 3 months (Dorey 2005), an increase of more than 4x in ejaculatory control time (Pastore 2014) and faster recovery of continence after prostatectomy (Geraerts 2013). With 5 to 10 minutes a day.
Conclusion
The male pelvic floor is not an abstract concept or one relevant only to older men. It is a concrete, trainable muscle group, directly responsible for functions that matter at any age. Understanding its anatomy is the first step. Strengthening it with a structured program like Ritmo is the action that transforms.